The cost of a mobile clinic feels huge when you’re the one who has to explain it to your board. You might sit in your office in Cleveland or Fresno and think, how do I get everyone to see what I see? You know care is slipping through the cracks.
There’s a good chance you see missed appointments, long drives, and whole neighborhoods with zero access to help. You also see the risk of doing nothing. People stay sick. Small problems grow into big emergencies. Your team burns out. The gap between the care people get and the care they deserve keeps growing, and it weighs on you. You want a way to bring real support right to folks who struggle with distance, cost, or trust. A mobile health clinic feels like the path that closes that gap and brings you to a future that feels a lot more hopeful.
AVAN Mobility has spent over 10 years building mobile medical clinic vehicles for programs across the U.S. Our team has built over 150 mobile medical units that help reduce barriers to care and save lives every day. We’ve supported groups like CalOptima, the Community Clinic of Southwest Missouri, and many more across the country. We take time to understand your goals and the people you care for. We want this article to serve you in a fair way since we know we aren’t the only option out there.
In this guide, you’ll get clear steps that help you make your case with confidence.
You’ll learn about:
- The state of healthcare in the U.S.: Why gaps keep growing in many counties.
- How to justify the cost of a mobile clinic: What leaders want to see.
What’s the real cost of people missing healthcare?
You see it every day in your community. People skip care because it feels too expensive or too far away. The cost of a mobile clinic starts to feel easier to explain when you look at the cost of people missing care. It hurts families, stretches your team, and drives spending higher for everyone. This is the gap many health leaders try to close, especially in states like Texas, Florida, and Alabama, where long drive times and low clinic access hit hard.
You might already feel the weight of this. Folks tell you they can’t take time off work. They can’t find a ride. They can’t pay for a visit. You know these barriers have real consequences. People end up sicker. They face more pain. They need more complex care later. It is tough to watch because these issues feel preventable.
Here’s what the data shows about missed healthcare in the U.S.:
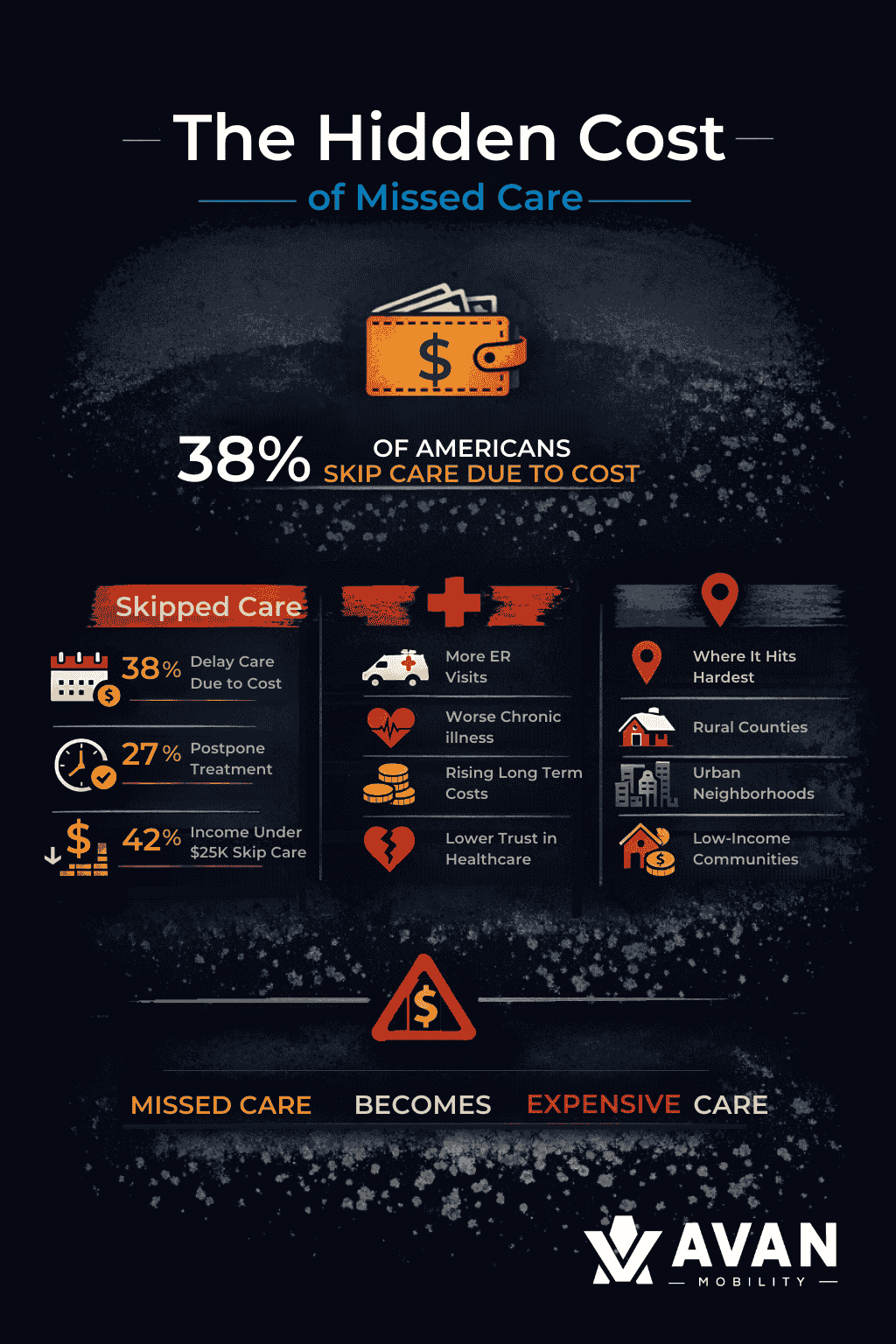
These numbers show how many people fall through the cracks. The financial impact stretches far beyond a missed appointment.
What can missed care lead to?
- Higher emergency visits: People show up in the ER for issues that a simple checkup could have caught.
- Worse chronic conditions: High blood pressure, diabetes, asthma, and heart disease grow harder to treat.
- Rising long-term costs: The CDC reports chronic conditions drive most of the nation’s healthcare spending.
- Lower trust: People lose confidence in local health systems when they can’t get basic help.
This hits rural counties in states like Montana and West Virginia the hardest. People may live an hour from the closest clinic. If they don’t have a car, the gap grows. In cities like Los Angeles or Houston, the problem shows up in a different way. People sit on long waitlists. Public transit takes too long. Life gets busy, and care gets pushed to the side.
You feel this pressure when your program has to stretch to meet everyone’s needs. Missed care becomes your problem even though you didn’t create it. Your staff gets tired. You get stuck reacting to crises instead of preventing them.
A mobile health clinic changes that picture. It meets people where they are, shrinks travel time, and builds trust because care becomes easier to reach. People get help early instead of late. The cost of a mobile clinic starts to look like an investment that pays off in healthier communities, lower long-term spending, and a calmer workload for your team.
Next, we’ll look at how to explain this value to your board in a simple and clear way that shows the return on investment.
How do you justify the cost of a mobile clinic to your board?
When you bring the cost of a mobile clinic to your board, you want a clear way to show value. You want to explain the return, the risks of staying the same, and the impact a mobile health clinic can make for your community. Your board wants facts, numbers, and a plan. You want them to feel the real need you see every day. This section helps you do both.
Start with the number. A Mobile Clinic Van typically costs between $170,000 to $290,000. Use that figure upfront so your board hears the plain cost, and then you can tie that cost to real savings and real outcomes.
Lead with a simple financial frame
Boards like short math. Give them three clear lines of reasoning:
- One-time capital: $170,000 to $290,000 purchase price, as mentioned above.
- Per-visit cost: Mobile clinic visits can cost a small fraction of an emergency room visit, sometimes under $50 per visit. That contrasts with ER costs, which are roughly $1,000 to $1,700, depending on source and case mix. often in the hundreds or thousands per visit. Use $100 as a conservative program average for mobile clinic visits and a conservative $1,200 for ER visits.
- Return on investment: Research has shown mobile clinics can generate large savings by avoiding ER care, and one review put savings as high as $36 for every $1 spent when comparing mobile visits to emergency visits. Use that as a top-line claim and show local math after.
- $1,200 minus $100 equals about $1,100 saved per person who would otherwise use the ER. That is the kind of number boards get.
- If your mobile clinic sees 300 unique patients per month, that is 3,600 visits a year. If just 10 percent of those visits avoid an ER trip, that is 360 avoided ER visits. At $1,100 saved per visit, that equals $396,000 in avoided costs for the year. This single example can cover the purchase in the first year, and then continue to pay back in the following years.
Show program revenue and funding streams
Boards worry that mission costs will drain the budget. Show possible offsets.
- Billing and reimbursements: Many mobile clinic visits can be billed to Medicaid, Medicare, or private insurance when licensing and staffing match payer rules.
- Grants and awards: Federal and state grants, including HRSA programs, often fund mobile clinic projects or pilot programs. Search local grant pools and state health department funding.
- Partnership dollars: Local health systems, hospitals, or insurers sometimes contribute outreach funding to reduce avoidable hospital use.
- Philanthropy and one-time capital: Foundations and donors often fund capital purchases, reducing your board’s direct capital burden.
Tie health outcomes to dollars
Connect clinical impact to cost savings. Use national cost drivers to show the stakes.
- Chronic disease costs: Diabetes care and complications cost the U.S. hundreds of billions per year, with average annual medical spending for a person with diagnosed diabetes near $20,000. Early screening and basic management reduce those costs.
- Emergency care cost burden: Emergency and inpatient care drive a lot of high-cost spending. Preventing hospitalizations and ER visits directly lowers community costs.
Use local data and a small pilot test to prove it
Boards love pilot tests. Offer a short, low-risk test that shows real results.
- Pilot idea: Run the mobile clinic 2 days a week in a high-need neighborhood for 6 months.
- Metrics to track: Visits, number of avoided ER referrals, billing revenue, patient satisfaction, and reduction in no-show rates at partner clinics.
- Simple target: If the pilot project sees 200 patients per month and avoids 5 percent of ER visits, show the board the projected avoided cost number and the expected break-even date.
After the numbers, give one brief example that matters to your board and puts a face to the math:
- Example: A single avoided hospitalization for uncontrolled diabetes can save multiple thousands of dollars and keep a parent working and kids in school. That is the kind of ripple effect your board values.
Close with a clear ask
End your board packet with a simple set of asks:
- Approve pilot funding: $X for 6 months of operations.
- Authorize capital search: Approve exploring grants, loans, or lease options for the $170,000 to $290,000 purchase.
- Commit to 3 metrics: Visits, avoided ER events, and revenue collected.
This plan gives your board clear numbers, simple math, and a low-risk way to test the impact. It frames the cost of a mobile clinic not as an expense, but as an investment that reaches people, lowers high-cost care, and supports your mission.
Ready to take the next step with your mobile clinic investment?

You likely landed on this article because you needed some clarity on how to justify the cost of a Mobile Clinic Van to your organization. Now, you know the price range of a Mobile Clinic Van and how you can explain the impact, savings, and long-term value it can create for your community.
AVAN Mobility has helped organizations across North America launch programs that remove barriers to care. Our team builds vans that support real work in real communities, from rural towns to busy cities. We guide leaders through the entire process, from early planning to vehicle delivery, so they never feel lost or alone.
We do this work because access to care should not depend on your street address, and every clinic deserves a partner who takes that mission seriously. If you have questions, click the button below to talk to a mobility expert today.
If you’re not ready to talk to a mobility expert yet, here are some helpful resources to keep learning.
- Buying a mobile medical van: Your process with AVAN Mobility: This walks you through the buying journey so you know exactly what to expect next.
- Top 10 tips on fundraising for a Mobile Clinic Van: This gives you practical ideas to help secure funding and speed up your project.